The cornea (the clear window at the front of the eye) would be completely spherical in an ideal world however the great majority of people have some degree of astigmatism where the cornea is more rugby ball shaped. If you imagine a magnifying glass which is rugby ball shaped you will appreciate that it would be hard to focus the light properly and get a clear image. This astigmatism of the cornea causes blur and is corrected by spectacles. This astigmatism has an effect on vision on top of any long or short sightedness you may have.
We do some calculations to work out what power of lens to put into the eye to try and take away any long or short sightedness but if you are left with astigmatism that will mean that your unaided vision (vision without spectacles on) can still be sub-optimal.
Because astigmatism involves the cornea being more curved in one axis than the other (rugby ball shape), incisions can be used in the more curved axis to reduce the astigmatism so the cornea has a rounder shape (football). The procedure is called astigmatic keratotomy or AK and is available as an adjunct to your private cataract surgery. The aim is to make the cornea a better shape so that your vision without spectacles is better than it would be without addressing that.
I use a diamond blade to make specially placed incision in the cornea at the time of surgery. The placement and depth of the incisions is worked out using a special algorithm.
This technique can reduce a significant amount of astigmatism but the results can be variable as everyones cornea behaves differently.
Another alternative is to use a lens in the eye which counters the astigmatism of the cornea – a toric lens.
Extended Depth of Focus IOLs
Standard cataract surgery involves removal of the cloudy lens in the eye and replacing it with a synthetic lens. This lens is called an intraocular lens (IOL) and is usually calculated to set you for distance vision in the NHS. Most people are used to wearing reading spectacles and this does not trouble them but the effect on intermediate vision is often underestimated. It is frustrating to have to wear spectacles for your computer screen or tablet as well as for proper reading. When you are out shopping having to reach for reading spectacles to read the label is frustrating.
Extended Depth of Focus IOLs are the latest generation of premium intraocular lenses. They focus the light for distance just like the non-premium lens but they also use some light energy to give you clear vision for intermediate and, to some degree, near. They literally extend the depth of your focus/vision with minimal downside. We have the opportunity to transform the visual quality of life for the long term. These lenses can also correct any pre-existing astigmatism so even that is not a concern.
Patient satisfaction is extremely high.
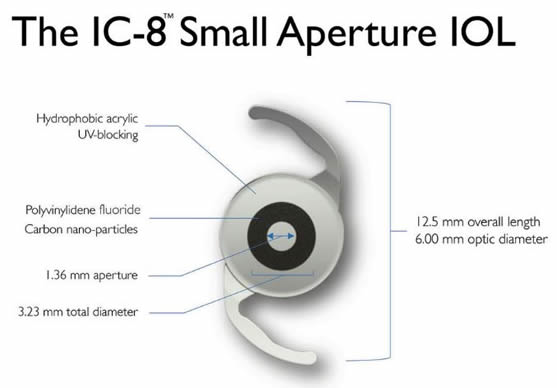
IC-8 pinhole IOL
IC-8 pinhole IOL
The AcuFocus IC-8 intraocular lens extends depth of focus by combining small aperture technology with a monofocal lens. This innovative design – incorporating an opaque mini ring with a central aperture – provides cataract patients with excellent quality of vision over a broad range of distances. It effectively mimics a pin hole camera to allow clear vision at multiple distances.
Essentially, the IC-8 IOL uses the pinhole effect to exclude peripheral defocused light – which compromises image quality – and permits only central, focused light to reach the retina thereby theoretically ensuring good vision at all distances.
Patients get less glare or other light related visual disturbance. Also it works in one eye allowing me to choose a lens which suits the individual patient in the other eye.
In general, the IC-8 IOL may be applied to cataract patients with up to 1.50 D pre-existing corneal astigmatism.
During cataract surgery, your eye's natural lens is removed and replaced with an intra-ocular lens (IOL). I will arrange for special investigations to work out what lens power to use. A standard monofocal lens will aim to give you great distance vision but it will mean that everything close up is blurry. You will require reading glasses for near vision such as reading and also for your intermediate vision, for example reading your tablet or computer. A multi-focal lens is designed to give you good near, intermediate and distance vision.
The technology is not perfect and it will not give you perfect distance and near vision but it should be pretty close. The vast majority of patients I have implanted with these lenses have found themselves independent of spectacles.
These lenses take the light energy and split it off into different focusing points. The brain gets two or three in focus images on the retina and it has to learn which one to notice and which to “see”. Once your brain adapts to the new way of seeing it will recognise what image it needs to use and ignore the other image(s).
Multifocal lenses deliver amazing results but they do have some compromises. They are not for everyone. We will need to decide together whether they are suitable for you once we assess your lifestyle, visual needs, clinical status and motivation for spectacle independence.
Premium Monofocal
Not truly a multifocal lens but a premium lens nonetheless. With ordinary NHS cataract surgery patients have a lens that sets them for distance. This is great for the majority but some patients struggle with intermediate vision; using the computer, seeing labels on food goods, seeing the speedometer in the car etc.
To address this Tecnis have developed the Eyhance Intraocular Lens™. It gives superb distance vision but also has a central segment with more power in order to allow a greater depth of focus.
Greater flexibility with vision has a big impact on quality of life.
It must be emphasised that these lenses do not give true distance and intermediate vision. They simply make the intermediate vision a bit clearer. For true distance and near/intermediate vision patients should opt for the other lenses detailed on this page.
I will now be implanting all my private patients who need monofocal lenses with the Eyhance Intraocular Lens™, a premium lens which delivers over and above the ordinary NHS lens.
Zeiss AT Lisa
The AT Lisa (Zeiss) has multiple concentric rings to focus the light in different places. It looks a bit like the glass lens you see on a lighthouse light. The presence of those concentric rings cannot be completely problem free and glare is almost inevitable but thankfully tolerable in the vast majority of patients. Also because the energy of the light is split/reduced for each focal distance it means that if you have any problem with the macula (such as age related macular degeneration/wear and tear) this is not the lens for you.
Zeiss AT Lara
This is a new lens from Zeiss which is described as an extended depth of focus lens (EDOF). Rather than splitting the light energy off into three distinct zones it blends the light energy over a greater depth of field. This gives you good distance and intermediate vision but near vision tends to be more of a struggle. This type of lens is ideal for those who want the benefit of a premium lens without the risk of visual side effects such as halos.
Precizon™ Presbyopia Correcting IOL
This is a refractive IOL and has separate distance and near segments in a new innovative design. It negates the potential glare and adverse light effects of the rings of some of the other premium lenses and transmits more light energy.
There are problems that can occur with multifocal lenses. Some patients get glare and some notice a reduction in light energy. One in a hundred patients may need their multifocal lens removed and replaced. In later life we are also more dependent on light energy so having a reversible procedure seems desirable.
To allow a safety net I have adopted the new DUET technique whereby a monofocal lens is placed into the usual position and a specifically designed multifocal lens is placed in front of that to facilitate the distance and near vision. This delivers the best of both worlds and allows us to remove the multifocal lens with ease in the future.
Looking for Perfection?
If you want perfection then these will not give it to you but they will give you good quality vision. If you want a compromise and get good near and distance vision with the potential of a few visual side effects which are usually not particularly troublesome then these lenses could be an option for you. I try my best to give some degree of spectacle independence however there are no guarantees. Even if things go completely to plan there are some patients that still require spectacles.
What You Should Know Before Considering a Multifocal IOL
Particularly with multifocal IOLs, you must be prepared for the possibility of at least some visual distortions — particularly in the form of glare and halos around light sources at night. These distortions rarely stop you night driving but in some people they can be annoying. If night driving is vital for you (for example if you are a lorry or taxi driver) then I would not recommend a multifocal lens.
Other reasons you may be eliminated as a candidate for multifocal IOLs include:
Astigmatism does not exclude you as toric lenses are available that correct the astigmatism for you by putting the astigmatism correction into the lens itself.
Other eye problems, such as retinal diseases, which would reduce the quality of your vision.
If you have already had cataract surgery but been left with poor near and/or intermediate vision and are thus still reliant on spectacles there is an option of putting another "top-up" intraocular lens into the eye to correct this without the need for spectacles - the Sulcoflex® Multifocal IOL.
Phakic IOLs – treatment for short sightedness
Phakic IOLs (intra-ocular lenses) are clear implantable lenses that are surgically placed either between the cornea (clear window at the front of the eye) and the iris (the coloured portion of your eye) or just behind the iris, without removing your natural lens.
This lens does the same job as spectacles or contact lenses do in focusing the light but it lies within the eye and does its work from there. It is designed to take away the need for spectacle wear. It is placed permanently but can be removed surgically at any time.
A phakic IOLs offer a permanent correction of short sightedness/myopia.
Unlike contact lenses, you can't feel a phakic intraocular lens in your eye and, apart from regular eye exams to monitor the position of the lens, the health of the undersurface of the cornea and to check the eye pressure, phakic IOLs typically do not require any maintenance.
I use two types of Phakic IOLs. One sits in front of the iris and the other behind the iris adjacent to the native lens in your eye.
Visian ICL
The Visian ICL (Implantable Collamer Lens) is a posterior chamber phakic IOL, meaning it is positioned behind the iris and in front of your natural lens. It is used for correcting nearsightedness ranging from -3.00 to -20.00 D.
Because the Visian ICL is placed behind the iris, it is undetectable to the naked eye and can only be seen through a microscope.
The Visian ICL is made of a soft, biocompatible collagen copolymer. Due to its flexibilty, the lens is able to be folded during implantation, allowing for a much smaller surgical incision.
AcrySof Cachet angle-supported phakic IOL:
The Cachet is a soft acrylic lens positioned in front of the iris and secured in the angle of the anterior chamber of the eye where the cornea and iris meet.
It can be used to correct short sightedness of -6.0 to -16.5 D.
Phakic IOLs versus LASIK Eye Surgery
Another frequently used option is to us LASIK laser treatment to correct short-sightedness.
It uses a computer-controlled laser to reshape the cornea.
There are some people who are better candidates for laser than a phakic IOL.
Contraindications to LASIK surgery include: a very high degree of nearsightedness (usually more than -8.00 D); having a cornea that is too thin or irregular in shape and eye conditions such as keratoconus and chronic dry eyes.
A 2010 study compared LASIK versus phakic IOL surgery for the correction of -6.00 to -20.00 D of short-sightedness (myopia) and found that the two procedures produced essentially equal odds of attaining 6/6 (20/20) perfect vision without corrective lenses one year after surgery.
The study also found that patients who underwent phakic IOL implantation had better contrast sensitivity and were more satisfied with their outcome than LASIK patients. Neither technique caused significant complications that permanently affected vision.
Risks and Complications
As with any type of surgical procedure, phakic IOL surgery has certain risks. Fortunately, these risks are low. Possible short-term and long-term complications of phakic IOL surgery include:
Retinal detachment, a serious and sight-threatening emergency situation.
Glaucoma, increased eye pressure that can damage the eye's optic nerve and cause permanent vision loss.
Loss of cells mining the inner surface of the cornea (endothelium) that could cause corneal swelling and progressive clouding of vision (I will have to do special tests at regular intervals to monitor the health of these cells).
This is an intraocular procedure and involved going into the eye so there is a very small risk of infection in the eye.
Distorted vision such as halos or glare, especially while driving at night, and blurry vision can occur.
As the synthetic lens is placed close to your native lens sometimes a cataract can form a few years earlier than it otherwise would. This can be corrected surgically if needed.

 Standard cataract surgery involves removal of the cloudy lens in the eye and replacing it with a synthetic lens. This lens is called an intraocular lens (IOL) and is usually calculated to set you for distance vision in the NHS. Most people are used to wearing reading spectacles and this does not trouble them but the effect on intermediate vision is often underestimated. It is frustrating to have to wear spectacles for your computer screen or tablet as well as for proper reading. When you are out shopping having to reach for reading spectacles to read the label is frustrating.
Standard cataract surgery involves removal of the cloudy lens in the eye and replacing it with a synthetic lens. This lens is called an intraocular lens (IOL) and is usually calculated to set you for distance vision in the NHS. Most people are used to wearing reading spectacles and this does not trouble them but the effect on intermediate vision is often underestimated. It is frustrating to have to wear spectacles for your computer screen or tablet as well as for proper reading. When you are out shopping having to reach for reading spectacles to read the label is frustrating. 
 The AcuFocus IC-8 intraocular lens extends depth of focus by combining small aperture technology with a monofocal lens. This innovative design – incorporating an opaque mini ring with a central aperture – provides cataract patients with excellent quality of vision over a broad range of distances. It effectively mimics a pin hole camera to allow clear vision at multiple distances.
The AcuFocus IC-8 intraocular lens extends depth of focus by combining small aperture technology with a monofocal lens. This innovative design – incorporating an opaque mini ring with a central aperture – provides cataract patients with excellent quality of vision over a broad range of distances. It effectively mimics a pin hole camera to allow clear vision at multiple distances.
 Not truly a multifocal lens but a premium lens nonetheless. With ordinary NHS cataract surgery patients have a lens that sets them for distance. This is great for the majority but some patients struggle with intermediate vision; using the computer, seeing labels on food goods, seeing the speedometer in the car etc.
Not truly a multifocal lens but a premium lens nonetheless. With ordinary NHS cataract surgery patients have a lens that sets them for distance. This is great for the majority but some patients struggle with intermediate vision; using the computer, seeing labels on food goods, seeing the speedometer in the car etc.
 There are problems that can occur with multifocal lenses. Some patients get glare and some notice a reduction in light energy. One in a hundred patients may need their multifocal lens removed and replaced. In later life we are also more dependent on light energy so having a reversible procedure seems desirable.
There are problems that can occur with multifocal lenses. Some patients get glare and some notice a reduction in light energy. One in a hundred patients may need their multifocal lens removed and replaced. In later life we are also more dependent on light energy so having a reversible procedure seems desirable. Visian ICL
Visian ICL
